

According to current estimates, the number of prescription opioid overdose deaths in the United States quadrupled between 1999 and 2010, and this increase occurred in parallel with prescription opioid sales. Studies have also linked the prescription opioid supply to opioid-related overdoses and mortality. As a result, researchers have suggested that it is possible that supply-based interventions may help in the fight against opioid misuse and abuse. However, some have proposed that reducing the prescription opioid supply may lead patients who are already addicted to opioids to substitute illicitly sourced prescription opioids or heroin, an illicit opioid.
A History Lesson
OxyContin is an extended-release formulation of oxycodone hydrochloride that is available in higher doses than immediate-release oxycodone. After it was introduced in 1995, it soon became an important drug of choice among people with substance use disorders. “The drug could be chewed and swallowed, or crushed then snorted, or injected to bypass the extended-release mechanism,” explains Marc R. LaRochelle, MD, MPH. “This enabled patients to obtain a quicker and more intense ‘high.’”
Propoxyphene is another agent that has been available for decades to treat pain, but this medication is a considerably weaker opioid analgesic than other agents in the drug class. Despite this knowledge, propoxyphene abuse cases were reported soon after its introduction, and it quickly became a leading agent in prescription drug–induced deaths.
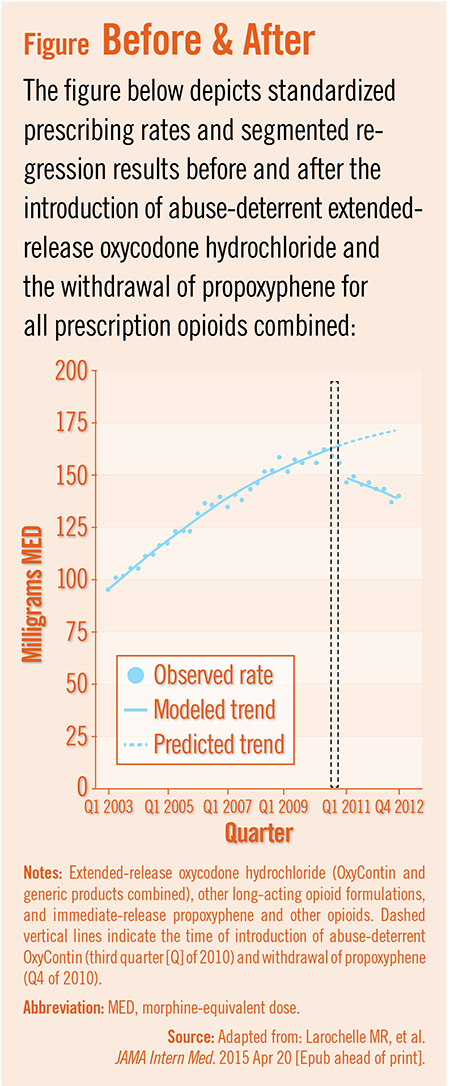
“In late 2010, two important changes occurred in the pharmaceutical market,” says Dr. LaRochelle. “The first was the introduction of abuse-deterrent OxyContin that was resistant to crushing, and the second was withdrawal of propoxyphene, which was found to have cardiac toxicity. By removing opioid formulations associated with increased risk, the hope was that the change would reduce opioid misuse, abuse, and overdose.”
Taking a Closer Look
In a study published in JAMA Internal Medicine, Dr. LaRochelle and colleagues assessed the link between the timing of the two opioid market changes—when abuse-deterrent OxyContin was introduced and when propoxyphene was withdrawn—with opioid dispensing and overdose rates from 2003 to 2012. The study group examined claims data on more than 31 million adult members of a national health insurer.
At 2 years after the opioid market changes, fewer prescriptions were dispensed for extended-release oxycodone, propoxyphene, and other immediate-release opioids. Total opioid dispensing decreased by 19% from the expected rate (Figure).
“Overall, the abuse-deterrent formulation of OxyContin resulted in 39% fewer prescriptions for extended-release oxycodone without an increase in alternative extended-release opioid formulations,” says Dr. LaRochelle says. “The sudden drop in dispensing for the abuse-deterrent formulation may have been due to decreased demand from those who were diverting or misusing the older, non-abuse-deterrent formulation.” He adds that there was no suggestion of a shift in formulary or out-of-pocket costs at the time of the formulation change.
In parallel with the decrease in opioid dispensing, the estimated overdose rate attributed to prescription opioids decreased by 20% when assessed at 2 years after the market changes. However, heroin overdose increased by 23% during that same timeframe. Dr. LaRochelle says that further studies are needed to understand the causes of the worsening heroin epidemic and to find ways to better treat patients who use it.
“What is clear from our study is that the introduction of abuse-deterrent OxyContin and the withdrawal of propoxyphene were associated with a decrease in both prescription opioid dispensing and overdoses,” Dr. LaRochelle says. He adds that pharmaceutical market interventions like these may be viable options to help reduce the epidemic of prescription opioid abuse. Opioid formulations that have been linked to high abuse potential or a narrow therapeutic window may represent model targets.
Examining the Implications
Results of the study may have significant implications for policymakers and healthcare professionals who are dealing with the opioid epidemic. “Imposing changes with regulatory mandates or voluntary pharmaceutical company actions will not, by itself, solve the drug abuse problem,” Dr. LaRochelle says. “However, it could be part of a multipronged approach to prevent or slow the number of new patients who become addicted to these agents.”
From a policy perspective, it is important to recognize how reducing the opioid supply affects access to these drugs among patients who may possibly benefit from them, says Dr. LaRochelle. “Furthermore,” he says, “prior to recommending abuse-deterrent formulations as first line therapy, we need to determine if they are safer than alternative, potentially less expensive opioids that are not prone to abuse.”
While restricting the opioid supply has the potential to decrease new-onset addiction in the future, Dr. LaRochelle cautions that such actions will not cure existing addiction. “The fact that heroin abuse is becoming more widespread shows that patients are likely to try to find alternatives,” he says. “We need to find ways to better identify and treat patients at risk of opioid abuse as well as heroin while at the same time ensuring that patients have access to the care they need.”
 PWeekly
PWeekly
{kind=link}