

Previous long-term research has found that there appears to be no difference in disease-free or overall survival between partial and total mastectomy for the treatment of invasive breast cancer. Despite these studies, substantial controversy remains regarding the definition of being free of tumor. “Until recently, no guidelines were available that described an adequate margin width for invasive or non-invasive breast cancer,” explains Lee G. Wilke, MD, FACS. “This lack of consensus has led to significant variations in reexcision rates for these patients.” She adds that the financial, psychological, and cosmetic effects of these repeat surgeries are important to patients and increase the burden of breast cancer therapy.
Identifying Key Determinants
In a study published in JAMA Surgery, Dr. Wilke and colleagues examined women who underwent initial breast conservation surgery (BCS) to determine the proportion that received a subsequent partial mastectomy or mastectomy. The study included more than 316,000 patients with stage 0 to II breast cancer who underwent initial BCS. Patients who were neoadjuvantly treated or whose conditions were diagnosed by excisional biopsy were excluded from the analysis. Information was collected from the National Cancer Data Base (NCDB), a large observational database of accredited cancer centers from the Commission on Cancer that contains data on more than 70% of patients treated for cancer in the U.S. The NCDB afforded an opportunity to observe differences among patient, tumor, and facility groups that were associated with repeat surgeries.
“Our results showed that about one-quarter of patients undergoing an initial BCS had at least one additional operation,” Dr. Wilke says. About two-thirds of this group had a complete lumpectomy while the remaining one-third received a mastectomy. The proportion of patients undergoing repeat surgery decreased only slightly during the 6-year study period. Several independent predictors of repeat surgeries were identified. These included age, race, insurance status, comorbidities, histologic subtype, estrogen receptor status, pathologic tumor size, node status, tumor grade, facility type and location, and volume of breast cancer cases.
Exploring Important Trends
The volume of breast cancer cases was minimally associated with repeat surgery rates unless high-volume institutions were examined. High-volume centers were 16% more likely to perform repeat surgeries than low-volume institutions. They were also more likely to be academic facilities. The authors noted that the repeat surgery rates observed among high-volume institutions may reflect patient referral patterns.
In addition, significant variations were observed in repeat surgery rates depending on the patient’s location in the country (Figure 1). Repeat surgeries were most common at facilities located in the Northeast when compared with facilities in the Mountain region. Academic or research facilities had a 26% repeat surgery rate, compared with a rate of slightly more than 22% that was seen at community facilities.
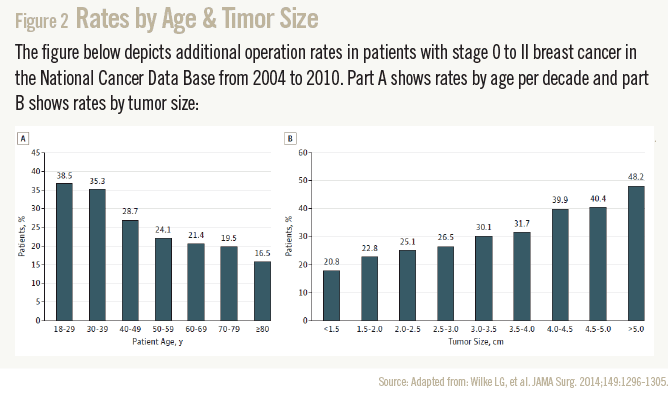
Researchers also found that the repeat surgery rate was nearly 39% for patients aged 18 to 29, compared with a nearly 17% rate that was seen among patients aged 80 and older. Larger tumor size was associated with a higher likelihood of repeat surgery. For tumors smaller than 1.5 cm, the repeat surgery rate was about 21%, compared with a repeat surgery rate of approximately 48% for tumors larger than 5 cm (Figure 2). In a multivariate regression analysis, patients with 2 cm to 5 cm tumors were 23% more likely to undergo repeat surgeries than those with tumors smaller than 2 cm.
More Work Needed
“Our data gives clinicians a starting point to begin improving rates of repeat surgery in breast cancer,” says Dr. Wilke. “One way to improve these rates is through standardization of an acceptable margin width as well as radiological and pathological processing of a BCS specimen.” The tumor margin width that can provide the lowest local recurrence rate has not been established in randomized controlled trials but has been evaluated via a large meta-analysis. Clinician should begin to implement use of the standard definitions of adequate margins as set in consensus guidelines by the Society of Surgical Oncology and the American Society for Radiation Oncology.
Dr. Wilke adds that clinicians need to incorporate the currently available consensus guidelines and conduct outcomes analyses of these recommendations to document a decrease in their own repeat surgery rates. “Our data should be used to better inform patients and providers about repeat surgery rates and how patient or tumor characteristics influence these rates,” she says. Through quality improvement projects, adoption of consensus margin guidelines and standardization of margin assessment, it is anticipated that the wide variation in repeat surgery rates will decrease as will the costs and patient anxiety surrounding tumor-positive margins.
 admin
admin
{kind=link}
{kind=link}