

The management of chronic non-cancer pain (CNCP)—defined as pain lasting beyond 3 months—has emerged as a significant challenge for healthcare providers throughout the United States. In recent years, some studies have suggested that opioids can be taken safely to manage several CNCP conditions for long periods of time and with few severe problems as long as they are well-selected. However, there is little specific guidance on the dosing of opioids for CNCP in any statutes, regulations, or clinical guidelines.
“Many pain specialists believe that the best way to manage CNCP is to increase the dose of opioids, a trend that has been increasingly prevalent throughout the U.S.,” explains Gary M. Franklin, MD, MPH. “But as this trend has continued, we’re seeing more frequent reports of deaths from accidental poisonings as well as problems with opioid abuse, dependence, and addiction. The CDC and other public health agencies have stated there has been an epidemic of opioid prescribing and adverse consequences from these practices since the late 1990s. Between 1999 and 2010, there were more than 100,000 opioid-related deaths in the U.S., which far exceeds the approximate 58,000 military casualties that the country endured during the Vietnam War.”
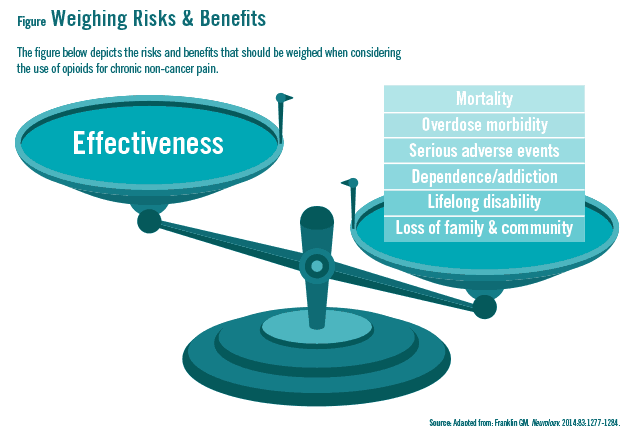
In the journal Neurology, the American Academy of Neurology (AAN) published a position statement, written by Dr. Franklin, to help physicians manage CNCP. The AAN is the first national professional medical association to adopt such a statement. “The evidence of harm associated with long-term opioid use is high while the evidence of effectiveness of this approach is low,” Dr. Franklin says. He notes that clinicians need to recognize this imbalance and weigh the risks and benefits when treating patients with CNCP (Figure).
Best Practices
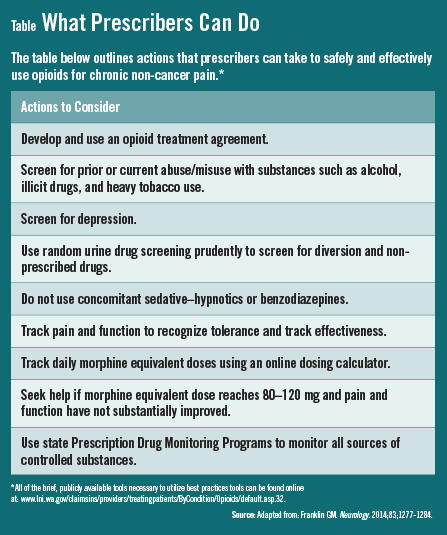
The AAN statement lists several best practices that clinicians can use to improve their use of opioids in patients with CNCP (Table). Some of these practices include using opioid treatment agreements with patients, accessing data from state Prescription Drug Monitoring Programs (PDMPs) before prescribing opioids, and routinely screening for substance abuse and mental health issues (see full study).
According to Dr. Franklin, one of the most important best practices from the AAN statement is to avoid escalating the dose of opioids, especially when patients are not achieving adequate pain relief. “It’s unlikely that chronic use of opioids for routine pain conditions like headache, fibromyalgia, and lower back pain will be worth the risk over the long haul,” he says. There is little evidence supporting the use of opioids chronically for conditions like migraine or generalized pain.
For more severe conditions—including destructive rheumatoid arthritis, sickle-cell disease, or severe neuropathic pain, among others—the AAN position paper recommends that prescribers seek out specific guidance on dosing opioids safely and use publicly available tools to effectively screen patients for opioid-related risks. Physicians also need guidance on how to monitor patients for early signs of severe adverse events, misuse, or opioid use disorder.
Alternatives to using long-term opioids for CNCP include cognitive-behavioral therapy, graded exercise, spinal manipulation, and interdisciplinary rehabilitation. “If CNCP persists, we can’t abandon these patients when they seek help,” says Dr. Franklin. “We need to use alternative treatments to more effectively relieve pain rather than continue to increase the use and dose of opioids.” He adds that physicians should also judiciously taper patients off opioids after they have been using higher doses for long periods of time, particularly if they have experienced an overdose event or if there is no evidence that pain and function have substantially improved while on opioids.
A Call to Action
The AAN position paper calls for primary care providers (PCPs) to refer chronic pain patients to specialists if they are taking high daily doses of opioids. “Opioid therapy should be part of a multifaceted approach to pain management,” says Dr. Franklin. “PCPs are often at the forefront, but using a collaborative care model can improve efforts to reduce opioid-related ED visits and hospitalizations. There needs to be active engagement within the community to ensure that opioids are being used appropriately.”
Dr. Frankin says that several approaches may further help PCPs with the appropriate use of opioids, including the integration of best practices into electronic health records, use of pharmacist co-management, and more widespread use of specialty consults via telehealth. “Time will tell if these types of interventions can improve how clinicians use opioids to manage pain,” he says. “In the meantime, physicians can refer to the AAN position paper to find information on the best practices for opioid use in patients with CNCP. There are many tools available, but the key is to get physicians to integrate them into their daily practice.”
 Janine Anthes
Janine Anthes
{kind=link}
{kind=link}