

Recently, the American College of Cardiology Foundation (ACCF) and American Heart Association (AHA) jointly released an expanded clinical practice guideline for the management of patients with heart failure (HF). The update, published in the Journal of the American College of Cardiology was designed to assist clinicians in selecting the best management strategies for patients. “The guideline updates definitions and classifications for HF, increases the emphasis on patient-centric outcomes, and introduces ‘guideline-
directed medical therapy’ (GDMT),” explains Clyde W. Yancy, MD, MSc, FACC, who chaired the ACCF/AHA writing committee.
Descriptions & Classifications of Heart Failure
The ACCF/AHA guideline update provides a more focused approach on dilated cardiomyopathies and the appropriate evaluation of patients. This includes family and genetic screening and counseling. “The guidelines once again endorse four stages of disease progression: Stages A thru D,” explains Dr. Yancy. “Stage A patients are those with positive risk factors, whereas Stage B patients have existing but still asymptomatic left ventricular function.”
“The expectations are highest for hospitalized patients with HF because of their vast resource consumption from initial admissions to subsequent readmissions.”
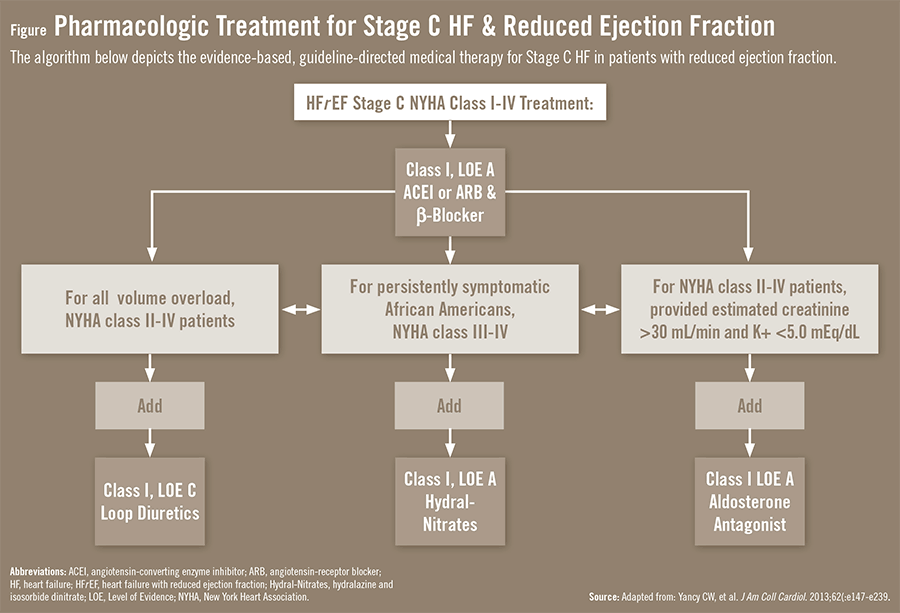
Stage C is the classic patient with congestive HF, but importantly, Dr. Yancy says this patient group is now well dichotomized as having HF with reduced ejection fraction (EF) or HF with preserved EF. “Best therapies are aligned with each stage, specifically risk factor modification, pre-emptive medical and device therapies for asymptomatic left ventricular dysfunction, and classic evidence-based therapies for symptomatic HF patients with reduced EF,” he says. “The guidelines also provide a treatment algorithm for Stage C HF patients with reduced EF [Figure]. The algorithm, known as GDMT, can serve as a decision tree that is more likely to lead to an effective medical regimen and increase the chances of optimizing patient outcomes.”

Stage D patients are those with advanced disease. For Stage D, the guidelines strongly support the use of left ventricular assist devices and referral for transplantation in carefully selected patients. However, there is equal endorsement for palliative care referrals and hospice as more patient-centric approaches when patients inform their clinicians of these preferences.
CRT/ICD Use in Heart Failure Patients
More discriminate use of cardiac resynchronization therapy (CRT) and implantable cardioverter-defibrillators (ICDs) is now recommended by the ACCF/ACC. “The decision to use CRT should be highly individualized and involve both best interpretation of available evidence and patient preference,” says Dr. Yancy. “Patients should be considered for CRT if they have an EF lower than 0.35, widened QRS, and are already on GDMT. As a performance measure, it’s imperative that patients be made aware of their risk of sudden death. An ICD should be considered if patients have a low EF despite receiving GDMT and have a life expectancy of at least 1 to 2 years. Device therapy isn’t for everyone, so it’s important to utilize it in those who are most likely to respond best to it.”
Reducing Hospital Readmissions
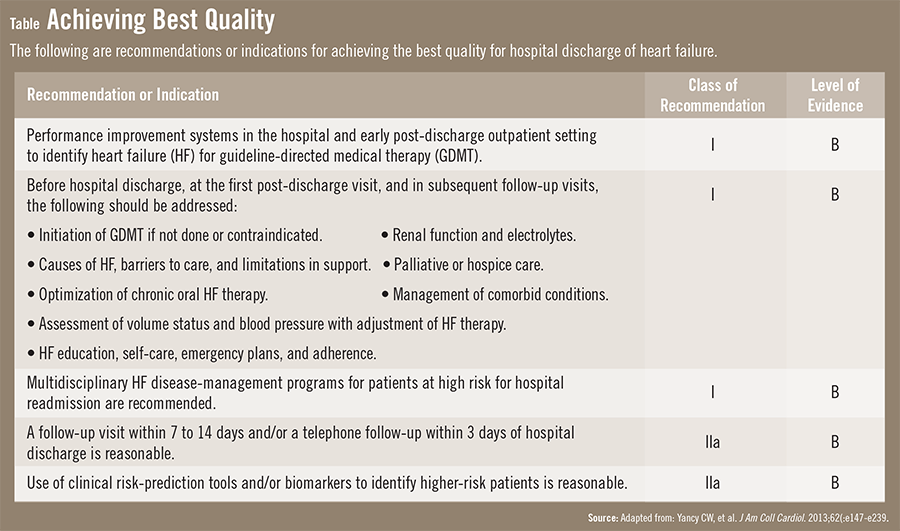
Healthcare is increasingly becoming an outcome-driven industry. Dr. Yancy says that this has led to clinicians being held accountable for providing the best quality and the best outcomes. “The expectations are highest for hospitalized patients with HF because of their vast resource consumption from initial admissions to subsequent readmissions.” The guidelines offer several straightforward interventions that are evidence-based and proven to be effective (Table). Notably, early telephone calls and follow-up and office visits with a healthcare provider within 1 to 2 weeks are recommended to reduce readmissions for HF.
Eyes on the Future of HF Care
Despite the wealth of currently available evidence, significant gaps in knowledge remain on many fundamental aspects of HF care, such as an effective management strategy for HF patients with preserved EF. Also lacking are data to support the use of biomarkers in optimizing medical therapy and the critical need for improving patient adherence to therapeutic regimens. More studies on patient-centered outcomes research may help address some of these deficiencies.
“We still need to learn more about successful risk modification, sophisticated screening, and effective treatment interventions that reduce the progression of HF,” says Dr. Yancy. “We’re continuing to increase knowledge about and treatment for HF in those with preserved EF, but more work is needed. Greater attention on the management of comorbidities is also necessary. For now, the emphasis in the ACCF/AHA guidelines on quality of care and performance improvement is well-placed and should be firmly embraced by those who see and treat patients with HF.”
 admin
admin
{kind=link}
{kind=link}