

Physical disability and loss of independence can complicate the care of patients with heart failure (HF) and worsen their quality of life. The ability to perform activities of daily living (ADLs) is often used to measure functional disability. ADLs include daily self-care activities that patients would routinely perform at home or when interacting with external environments. However, it can be challenging to estimate functionality through patient-reported outcomes using ADLs.
“Little is known about the prevalence of ADL deficits and functional disability in patients with HF,” says Shannon M. Dunlay, MD, MS. “Having a limited understanding of this relationship in patients with HF is problematic because disease-specific treatment options often depend upon a person’s functional capabilities.” The association between functional disability and outcomes such as mortality and hospitalization in patients with HF is also unclear. To address this research gap, Dr. Dunlay and colleagues had a study published in Circulation: Heart Failure. They investigated the prevalence and progression of difficulty with basic and instrumental ADLs in patients with HF.
Functional Difficulty Common
For the study, more than 1,100 patients with HF who were an average age of 75 were classified as having minimal, moderate, or severe difficulty with ADLs, such as getting dressed, cleaning the house, climbing stairs, taking medications, and using the bathroom. Nearly 20% of HF patients were obese and most had other comorbidities, such as hypertension, anemia, and diabetes. “Almost 60% of patients had difficulty with one or more daily tasks at the start of the study,” Dr. Dunlay says. “About 24% had moderate difficulty with ADLs while nearly 13% had severe difficulty.”
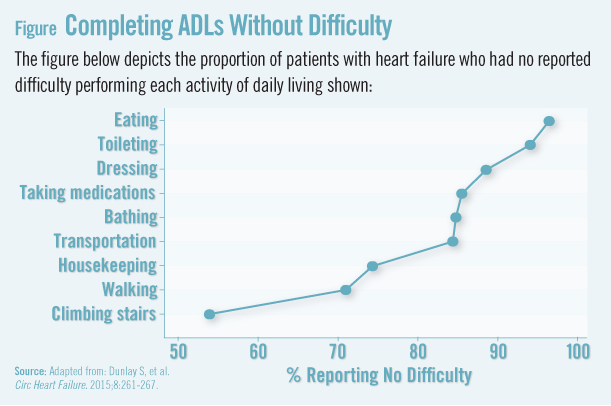
Results also showed that older women, unmarried patients, and those with obesity, diabetes, or anemia had more difficulty with ADLs and mobility. HF patients with dementia had difficulty with twice as many ADLs as others. The difficulty hierarchy of the nine ADLs assessed in the study was—in order from easiest to most difficult—eating, toileting, dressing, taking medications, bathing, transportation, housekeeping, walking, and climbing stairs (Figure 1). This hierarchy of difficulty may help clinicians assess current levels of function and provide insights into the types of activities that represent signs of decline or improvement in function.
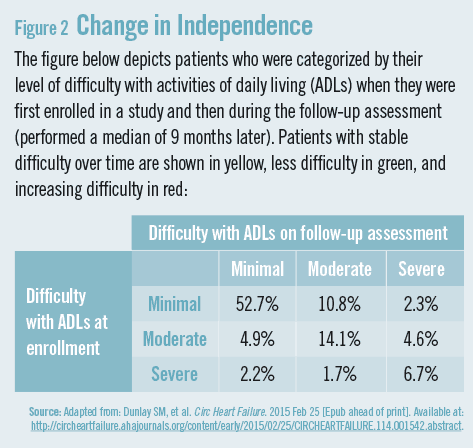
Over time, the level of ADL difficulty was stable in most patients (Figure 2). Only a small fraction improved, but nearly 18% worsened over time. Dr. Dunlay notes that the difficulty patients had with ADLs was probably not entirely attributable to HF. “Most patients with HF are elderly and have several other chronic conditions,” she says. “These comorbidities can have an impact on mobility and the ability to perform self-care activities. Based on our results, we need to find strategies to provide more comprehensive care to patients with HF.”
Hospitalizations & Survival
During about 3 years of follow-up, the vast majority of HF patients in the study were hospitalized at some point, and almost 55% of patients died. HF was the most common cause of hospitalization, followed by heart rhythm disorders and pneumonia. While most patients reported similar functionality 1 year later, persistently severe or worsening difficulty with ADLs was associated with higher mortality and increased risk of hospitalization. The average length of survival was approximately 6 years for those with minimal difficulty with ADLs, 3 years for those with moderate difficulty, and 1.5 years for those with severe difficulty.
Some patients experience a progression in functional disability over time, highlighting the importance of anticipating the needs of patients to provide patient-centered care. “Patients place a high value on functional independence, but increasing difficulty with ADLs can worsen quality of life, which can in turn affect disease management and impact outcomes,” says Dr. Dunlay. “Our findings should be viewed as a call to action to increase efforts to determine if specific interventions can help prevent the progression of functional disability in patients with HF.”
Assess ADLs Routinely
Dr. Dunlay says that ADLs can be easily assessed during office visits and may be helpful when discussing prognosis. “We can use information about functionality to inform patient-provider discussions about goals of care and expected functional trajectories,” she says. “If patients are having difficulty with one or more ADLs or have experienced worsening mobility over time, these events can serve as a trigger to pursue more thorough assessments and physical therapy evaluations. By enhancing our predictive capabilities and developing targeted interventions, we may help reduce the burden of ADLs in this patient group and improve upon outcomes in HF.”
 admin
admin
{kind=link}
{kind=link}