

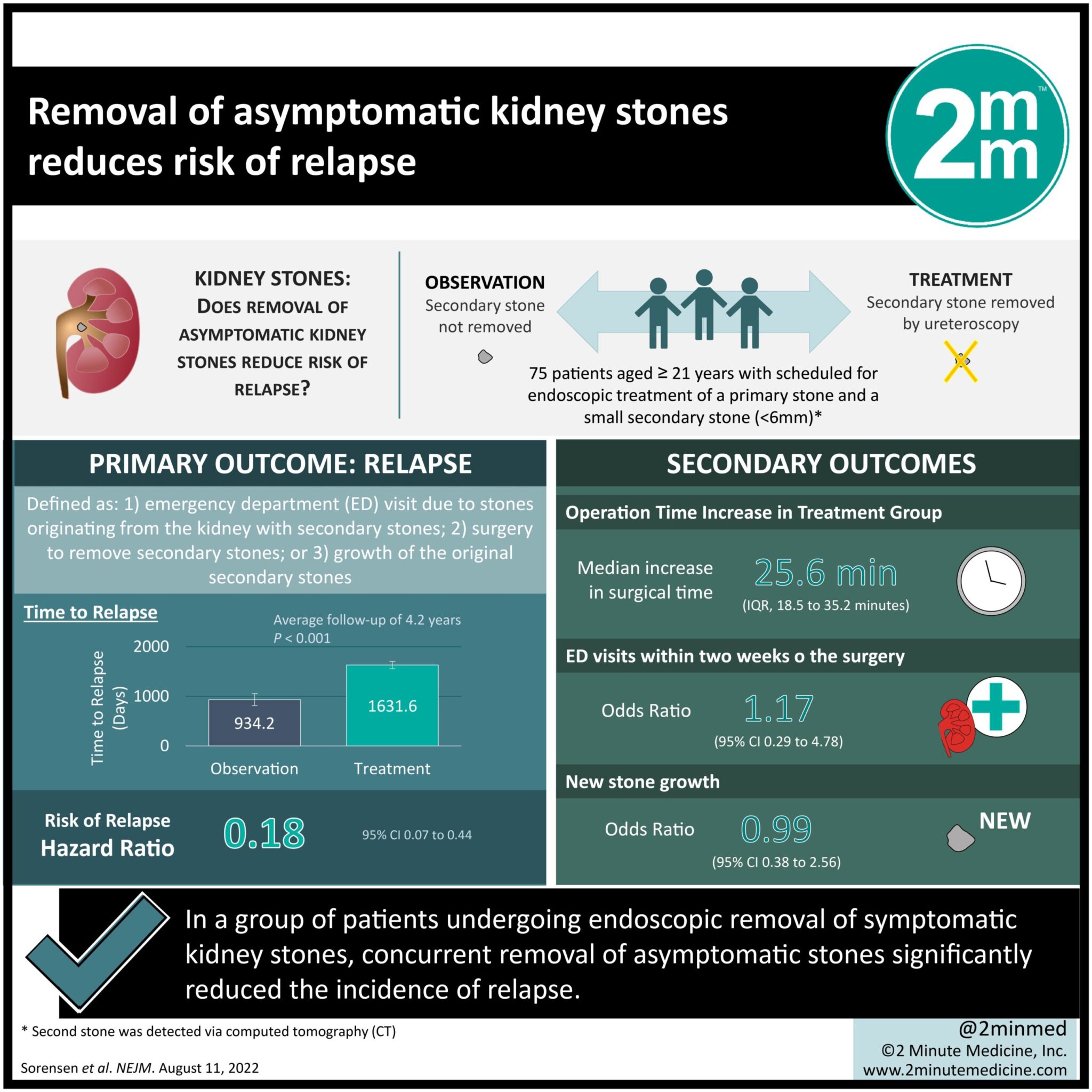
1. In a group of patients undergoing endoscopic removal of symptomatic kidney stones, concurrent removal of asymptomatic stones significantly reduced the incidence of relapse.
2. Concurrent removal of asymptomatic stones did not increase the number of emergency department visits after surgery.
Evidence Rating Level: 1 (Excellent)
Study Rundown: Symptomatic stones in the kidney or ureters are frequently removed endoscopically. During these procedures, smaller asymptomatic stones are often noted on imaging. Guidelines are unclear about whether to remove or observe these stones. A prospective study involving shockwave lithotripsy and previous retrospective studies supported observation. Nevertheless, approximately 50% of these small stones become symptomatic within five years of initial surgery. The present study was a multicenter, randomized, controlled trial where patients undergoing endoscopic removal of stones in the ureter or contralateral kidneys had their small, asymptomatic stones removed (treatment group) or observed (control group). The treatment group was found to have a longer time to relapse and a lower incidence of relapse within an average follow-up of 4.2 years. The two groups had no difference in emergency visits relating to the surgery. Despite its small sample size and lack of sub-analysis of surgical technique variability, this study provided the first prospective evidence of the potential benefits of pre-emptive removal of asymptomatic stones in reducing relapse risk.
Click here to read the study in NEJM
In-Depth [randomized controlled trial]: This randomized controlled trial assessed outcomes associated with concurrent pre-emptive removal of small, asymptomatic renal stones during endoscopic surgery for symptomatic stones. Patients were screened for inclusion if they were 21 years of age or older, scheduled for endoscopic treatment of a primary stone, and had small secondary stones (<6mm) detected via computed tomography (CT). In total, 75 patients were randomized 1:1 to have the secondary stones removed by ureteroscopy (treatment group) or observed (control group). The primary outcome was relapse, defined as: i) an emergency department visit due to stones originating from the kidney with secondary stones (trial side); ii) surgery to remove stones on the trial side; or iii) growth of the original secondary stones. After an average follow-up of 4.2 years, the treatment group had a significantly longer time to relapse (1631.6±72.8 days [mean ±standard error]) compared to the control group (934.2±121.8 days; p<0.001). The risk of relapse was 82% lower in the treatment group (Hazard Ratio 0.18; 95% Confidence Interval [CI], 0.07 to 0.44). The pre-emptive removal of secondary stones added a median of 25.6 minutes to the operation. Emergency department visits within two weeks of the surgery occurred in 13% of the treatment group and 11% of the control group (Odds Ratio [OR], 1.17; 95% CI, 0.29 to 4.78). New stone growth was detected via imaging in the same proportion (37%) of the treatment group and the control group (OR, 0.99; 95% CI, 0.38 to 2.56). In summary, this trial provided the first evidence to support the pre-emptive removal of asymptomatic stones during endoscopic removal of primary stones.
©2022 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.